Patient programs live or die in the first few minutes. If the enrollment experience feels confusing, overly invasive, or vague about how communications will work, patients abandon the flow and your brand loses the chance to provide education, support, and adherence help.
This article is for US pharma brand teams, omnichannel leads, commercial ops, marketing ops, CRM owners, and agency partners who design or run patient education and support journeys. You will learn how to build a consent-forward patient enrollment journey that improves patient program sign ups, reduces compliance risk, and creates cleaner data for patient engagement workflows and measurement.
Why patient enrollment journeys break (and why “more traffic” does not fix it)
Most enrollment drop-off is not caused by lack of intent. It is caused by friction and distrust: unclear permissions, too many fields too early, and uncertainty about whether the program will spam patients or expose sensitive health data.
In pharma, this is amplified by regulatory and reputational stakes. Even when a specific rule does not apply to every program, patients still expect healthcare-grade clarity and control, and internal reviewers often slow down launches when consent language is ambiguous.
- Permission ambiguity: “I agree” can mean enrollment, marketing consent, HIPAA authorization, and channel opt-in all at once.
- Early data asks: Collecting full profiles up front increases abandonment and creates unnecessary risk.
- Channel mismatch: Patients may want email education but not SMS, or vice versa.
- Fragmented systems: Consent captured in one place and messaging sent from another leads to preference drift and audit gaps.
What “consent-forward marketing” means in a patient enrollment journey
Consent-forward marketing treats permissions as a product feature, not a legal checkbox. In practice, it means patients can understand, choose, and change how they hear from you, without needing to call a support line or decipher fine print.
A consent-forward patient enrollment journey typically separates four things that are often incorrectly bundled:
- Program enrollment: joining the service or support experience.
- Data permission: what information is collected and how it is used.
- Channel opt-in: which channels are allowed (patient education SMS email, phone, mail).
- Content preferences: what topics and cadence the patient wants (lifecycle messaging healthcare vs. only key reminders).
What changed: why clearer permissions now drive both compliance and performance
Three shifts are pushing teams toward patient preference management and “clear permission UX” as a growth lever, not just a review requirement.
First, regulators have been explicit that health-related services outside HIPAA can still trigger privacy obligations. The FTC’s Health Breach Notification Rule is a reminder that patients’ health data expectations extend beyond traditional covered-entity contexts.
Second, SMS has moved from “nice to have” to core lifecycle orchestration, which raises the bar on opt-in and opt-out discipline. The FCC’s consumer guidance on unwanted robocalls and texts highlights the expectation that people control whether they receive marketing texts and can stop them easily.
Third, patient communications are increasingly treated like regulated brand experiences. Even when you are focused on education and support, teams often align experiences to the principles behind FDA oversight of prescription drug advertising and promotion, because unclear intent and inconsistent disclosures create review delays and operational risk.
The consent-forward enrollment blueprint (a practical UX model)
High-performing patient journey optimization starts with a simple idea: earn the next piece of data and permission step by step. The goal is not to collect everything. The goal is to get a confident “yes” to the right things, then grow the relationship.
Stage 1: Start with a “value-first” entry point
The first screen should answer three questions in plain language: what the program is, who it is for, and what happens after sign-up. If a patient cannot predict the next step, they hesitate or bounce.
- Lead with outcomes patients care about (education, affordability, reminders, nurse support) before forms.
- Use one primary action (for example, “Get started”) and one secondary action (for example, “Learn what you’ll receive”).
- Keep brand/legal detail accessible, but not in the critical path.
Stage 2: Confirm eligibility with the minimum viable data
Eligibility checks are often necessary, but they are also where many journeys over-collect. Ask only what you need to route correctly, and defer the rest until the patient sees immediate value.
- Progressive profiling: collect more information after the first useful interaction.
- Explain “why” inline: one sentence can reduce suspicion (“We ask this to confirm you can receive program benefits”).
- Offer a “save and continue later” option when the flow is longer than two minutes.
Stage 3: Separate enrollment consent from communications consent
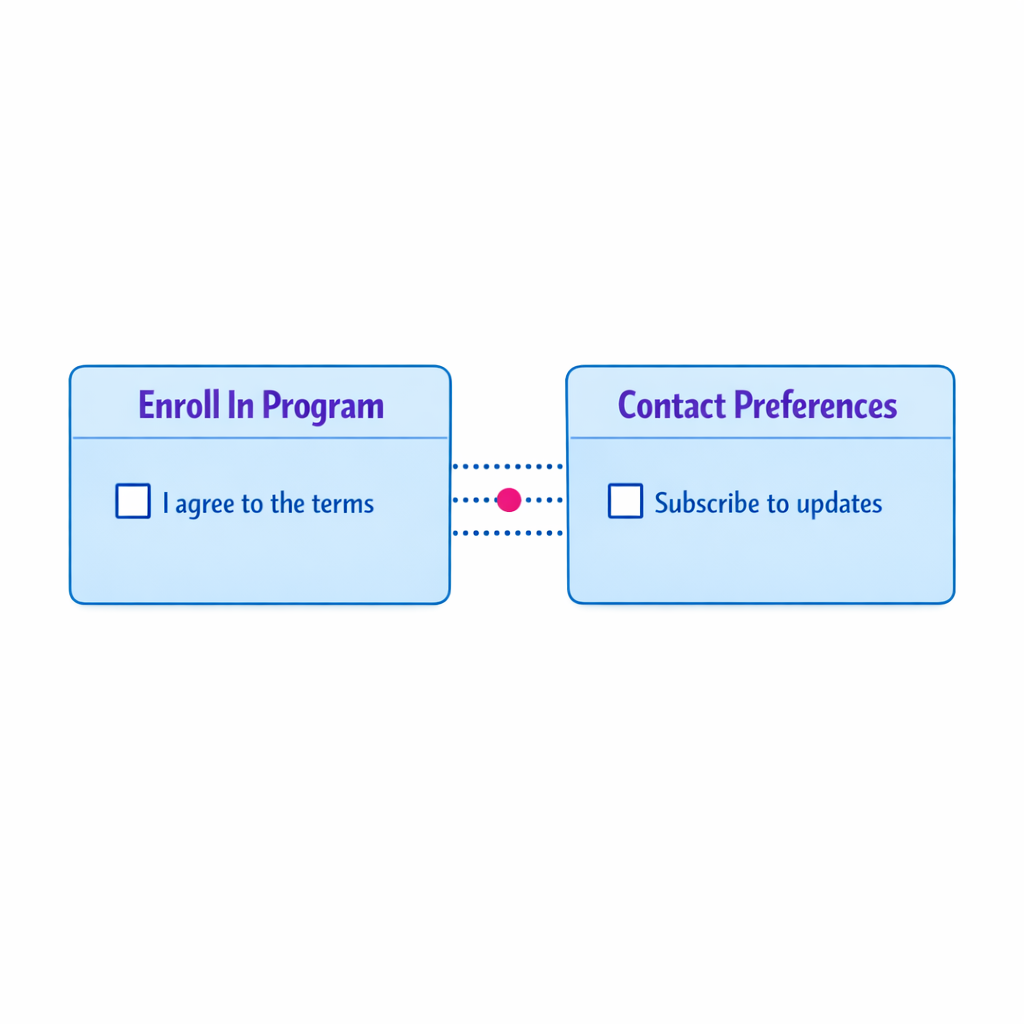
A common failure mode is treating program participation as automatic consent for ongoing messaging. That creates complaints, opt-outs, and internal escalation when downstream teams cannot prove what the patient agreed to.
Design pattern: two clear decisions with distinct labels.
- Decision A: “I want to enroll in the program.”
- Decision B: “Here is how you may contact me (and about what).”
When HIPAA-covered partners or PHI are involved, consent and authorization can be especially sensitive. The HHS guidance on HIPAA and marketing is a useful reference point for how “marketing” and authorization concepts differ from operational communications, and why clarity matters.
Stage 4: Capture channel opt-ins with explicit, patient-readable language
Channel opt-in is not just a compliance artifact. It is a deliverability and experience control system. If patients select their preferred channel at enrollment, you reduce suppression-list churn later.
- SMS: describe frequency ranges, what “STOP” does, and what kinds of messages will be sent.
- Email: clarify whether content is educational, adherence, savings, or brand news.
- Phone: indicate whether calls are live, automated, or both (if applicable).
For commercial email, the FTC’s CAN-SPAM Act compliance guide is a helpful baseline for expectations around identification and unsubscribe mechanisms, even when your content is largely educational.
Stage 5: Confirm preferences with a “receipt” screen and a self-serve preference center

After submission, show a confirmation that reads like a receipt: what the patient signed up for, which channels were enabled, and how to change it. This reduces support burden and prevents the “I never opted in” experience.
- Provide a single link or route to adjust preferences.
- Echo the chosen channels and topics in plain language.
- Set expectations for timing (“You’ll receive your first message within X days”) without overpromising.
Patient preference management: from static checkbox to living consent record
Preference management is often treated as a one-time capture. In reality, it is a lifecycle capability that needs to update whenever a patient’s situation changes: new therapy stage, new questions, or channel fatigue.
Operationally, strong patient preference management usually includes:
- A single source of truth for consent and permissions (not just CRM notes).
- Event-based updates (opt-in, opt-out, topic change, bounce, complaint, do-not-contact).
- Time-stamped records that show what the patient saw and selected at the moment of consent.
- Policy-aware routing so messages only send when the right permission exists.
This is where platforms and process design meet. A modern workflow tool can help orchestrate patient engagement workflows across SMS and email while keeping the consent state consistent, so brand, agencies, and ops teams do not have to manually reconcile lists.
How to design patient education SMS and email without damaging trust
Patients judge programs less by message creativity and more by whether messages feel expected. “Expected” is the product of clear permission language, recognizable sender identity, and consistent cadence.
Use “purpose-based” topics instead of channel-only choices
Many preference centers only ask “email or SMS?” Patients think in purposes: education, reminders, savings, next steps. Purpose-based options improve patient journey optimization because they align content with intent.
- Education: “tips, how-to content, and what to expect.”
- Reminders: “refills, appointments, or routine check-ins.”
- Support: “help getting started, navigating coverage, or connecting to resources.”
Make frequency a choice, not a surprise

If you cannot offer precise frequencies, offer ranges. “Up to 4 messages per month” is easier to trust than “periodic updates,” because patients can predict the impact.
Write consent microcopy like UX, not like legal
You still need review-grade language, but patients should not need to interpret it. Put the human explanation first, then provide expandable detail or a linked policy page in your actual implementation.
- Good: “Choose how you want to get updates. You can change this any time.”
- Risky: “By providing your number you agree to receive communications.”
Measurement: what to track in a consent-forward enrollment journey
Consent-forward marketing should produce measurable lift, but only if you instrument the journey. The goal is to connect UX and permissions decisions to operational outcomes: more completed enrollments, higher reachable audience, and fewer complaints.
Metrics to consider across the patient enrollment journey:
- Enrollment conversion rate: started vs. completed sign-up.
- Step-level drop-off: which screen causes abandonment (permissions screens are often the culprit).
- Permission yield: percent of enrollees who opt into at least one channel.
- Channel mix: SMS-only, email-only, both, or neither (and how it changes over time).
- Time to first value: time from sign-up to first helpful message or action.
- Opt-out and complaint rates: leading indicators of expectation mismatch.
- Preference edits: evidence that patients are using self-serve controls (a healthy sign).
In practice, the most useful view is a funnel that includes both conversion and permission states. A high enrollment rate with low opt-in rates can be less valuable than a slightly lower enrollment rate with strong opt-in patient communications.
Common mistakes and misconceptions (and how to fix them)
Mistake 1: Bundling all consent into one checkbox
Bundling looks efficient, but it increases distrust and creates downstream ambiguity. Split enrollment from channel consent, and split channels from topics when possible.
Mistake 2: Pre-checking opt-ins or hiding choices in dense text
Dark patterns may increase short-term opt-in, but they usually increase opt-outs, complaints, and internal risk. Consent that is not understood is not durable.
Mistake 3: Treating “education” as automatically exempt from messaging rules
Patients experience messages as messages, regardless of internal classification. Use the spirit of established guidance like the FCC’s resources on calls and texts to design obvious opt-outs and patient-controlled permissions, even for supportive content.
Mistake 4: Failing to synchronize opt-outs across systems
If a patient opts out via SMS but still receives email, they lose trust. Ensure every channel’s suppression and preference updates propagate to every sending system.
Mistake 5: Over-collecting data “because analytics might need it later”
Collect what you can justify. Over-collection increases abandonment and expands the sensitivity footprint you must protect.
Patient support program best practices: a practical build checklist
Use this checklist to evaluate and upgrade your current flow. It is designed for brand, ops, CRM, and agency teams to align quickly on what “good” looks like.
- Map the journey: document every step from entry point to first ongoing message, including handoffs between vendors and systems.
- Define permissions: explicitly separate program enrollment, data permission, channel opt-in, and topic preferences.
- Reduce first-step fields: keep initial enrollment to only what is required to start value delivery.
- Implement a preference center: make it easy to edit topics, channels, and cadence in one place.
- Standardize message expectations: sender identity, frequency ranges, and “what you’ll get” language.
- Instrument step drop-off: track abandonment and run structured tests on the highest-friction screens.
- Build an audit trail: store time stamps, consent language versions, and the patient’s selections.
- Align review early: bring legal, regulatory, privacy, and medical review into the UX model before creative execution.
Where Pulse Health fits: orchestration that keeps consent and UX aligned
Consent-forward enrollment journeys are hard to scale when permissions live in one tool, messaging runs in another, and measurement sits somewhere else. A platform approach can help teams centralize consent states, manage patient preference management, and orchestrate patient engagement workflows without rebuilding the same logic for every program.
If you are evaluating how to simplify enrollment, improve opt-in patient communications, and operationalize lifecycle messaging healthcare with cleaner measurement, Pulse Health can be a useful starting point to review your current flow and identify quick wins.
Request a Demo to review your enrollment journey and permissions model
If you want to pressure-test your current patient enrollment journey, walk through a consent-forward UX pattern, or discuss how to operationalize preferences across patient education SMS email and CRM, you can Request a Demo.
Prefer a working session with your team and partners? Book a Consultation to review your current funnel, consent language structure, and measurement plan.
If you are ready to align stakeholders on an orchestration approach, Talk to Pulse Health about how to turn permissions into a scalable foundation for patient journey optimization.