Patient education and enrollment programs often start strong and then stall at the exact moment that matters most: when a patient tries to sign up, give consent, and choose how they want to be contacted. For US pharma brand teams, omnichannel leads, commercial ops, and agency partners, that breakdown creates wasted spend, poor patient experience, and measurement gaps you cannot easily explain to stakeholders.
This article lays out a practical, scalable patient engagement journey that moves from signup to ongoing support while staying consent-first and compliance-aware. You will learn how to design a patient enrollment workflow, implement patient sign up best practices, operationalize consent management for healthcare marketing, and measure an opt-in patient communications program across channels, including SMS patient education.
Why “signup” is where patient engagement journeys usually fail
Most patient education campaigns focus on what to say, not how a patient actually enrolls. In reality, the enrollment moment is where friction, ambiguity, and trust concerns show up at once, especially if the patient is on a mobile device, anxious, or unsure what will happen next.
A scalable patient engagement journey treats enrollment as a product experience, not a form. That means you design it with clear value exchange, minimal steps, explicit choices, and a system that can prove what the patient agreed to and when.
Common failure patterns to watch for
- Consent is buried or bundled, so patients do not understand what they are opting into.
- Channel choices are missing, forcing “one-size-fits-all” outreach that drives opt-outs.
- Identity is brittle, so duplicates, mismatches, and incomplete profiles undermine measurement and orchestration.
- Support is disconnected, so patients fall into a dead-end after signup instead of entering a guided journey.
The compliance-aware baseline: what “consent-first” really means in pharma patient programs
“Consent-first” is both a trust strategy and an operational discipline. It means you only send what you are permitted to send, in the way the patient expects, and you can demonstrate it later if challenged by legal, compliance, or a partner audit.
Because program designs vary, teams typically align early on what is informational, what is promotional, and what is operational. That classification drives how you structure consent, how you document it, and how you route communications across email, SMS, and other patient outreach omnichannel touchpoints.
HIPAA: understand when communications become “marketing”
If your program involves HIPAA-covered entities or business associates, you should align stakeholders on how HIPAA treats “marketing” and what types of communications may require an authorization, using the HHS OCR guidance on the HIPAA Privacy Rule and marketing. Even when a message is permitted, patient expectations still matter, so the enrollment experience should clearly explain message types and frequency in plain language.
SMS and phone outreach: build for opt-in and defensible proof
For text messages and calls, teams typically design the patient enrollment workflow to capture the right consent language and retain evidence, because unwanted outreach is a high-risk failure mode. The FCC’s consumer guidance on stopping unwanted robocalls and texts is a useful baseline reference when aligning internal stakeholders on TCPA-driven expectations for consent, opt-out handling, and complaints.
Email: treat preferences and unsubscribe as product requirements
Email is often viewed as “easier,” but it still requires disciplined preference management and reliable unsubscribe handling. The FTC’s CAN-SPAM compliance guide provides a practical reference point for teams designing opt out patient communications flows and operational guardrails.
Electronic records and signatures: plan for auditability
If you are capturing electronic signatures or maintaining electronic records that need to be trustworthy and retrievable, your documentation approach should be deliberate from day one. FDA’s guidance on 21 CFR Part 11 scope and application is often used as a starting point to align on how systems, controls, and recordkeeping should support integrity and audit-readiness.
Promotion oversight: keep patient-facing experiences aligned with governance
Even when an enrollment flow is primarily educational or support-oriented, pharma organizations usually want governance that accounts for promotional risk and review pathways. FDA’s Office of Prescription Drug Promotion (OPDP) is a core reference for understanding the oversight landscape for prescription drug promotion and why consistent review processes matter.
What changed (and why teams are revisiting enrollment design now)

Many teams are reworking patient engagement journeys because privacy and sensitive-data expectations are tightening while patient patience is shrinking. Instead of treating compliance as a final review step, organizations are moving it upstream into experience design, data architecture, and measurement planning.
Two regulatory updates illustrate why “compliance-aware by design” is becoming the default in healthcare engagement clouds and patient access platforms. First, HHS OCR finalized updates that strengthen protections around reproductive health information, summarized in the OCR overview on HIPAA privacy guidance related to reproductive health. Second, HHS and SAMHSA finalized changes to modernize 42 CFR Part 2, which you can review in the Federal Register final rule on confidentiality of substance use disorder patient records.
Even if your current program is not directly in scope for these specific updates, they signal a broader trend: patient trust is increasingly tied to explicit choices, clear explanations, and the ability to honor preferences consistently across every touchpoint.
A scalable patient education & enrollment journey: the “signup to support” blueprint
A scalable patient engagement journey is not a single campaign. It is an enrollment workflow that turns intent into a permissioned, measurable relationship, then keeps that relationship useful through ongoing education and support.
Below is a blueprint you can adapt whether you are launching a new patient education campaign, improving an existing patient enrollment workflow, or building an omnichannel patient outreach motion across brand sites, hubs, call centers, and partner channels.
Stage 1: Entry points that set expectations (before you ask for data)

Patients often arrive from multiple places: brand sites, unbranded education hubs, HCP engagement pathways, call center referrals, or care-team prompts. Regardless of channel, the first screen should answer two questions clearly: “What do I get?” and “What will you do with my information?”
Patient sign up best practices at this stage are mostly about reducing uncertainty. Use plain language, avoid surprises, and keep the initial request minimal so the patient can say “yes” before they commit to a long form.
- Lead with value: what the program provides (education series, reminders, access support, nurse support, etc.).
- Explain the journey: what happens after enrollment, and how often you will reach out.
- Offer choice early: “email only,” “text only,” or “both,” when appropriate.
Stage 2: Consent capture that is explicit, modular, and durable
This is where consent management in healthcare marketing becomes a system, not a checkbox. Modular consent means the patient can opt into certain message types and channels without being forced into everything at once.
Design consent as a set of clear decisions a patient can understand. Then store those decisions in a way that downstream systems can act on without reinterpretation or manual cleanup.
- Separate purpose from channel: patients should be able to choose what they receive (education, reminders, support) and how they receive it (SMS, email).
- Capture the evidence: timestamp, source, version of disclosures, and any required language per channel.
- Make opt-out easy: preference changes should be as simple as signup, not a support ticket.
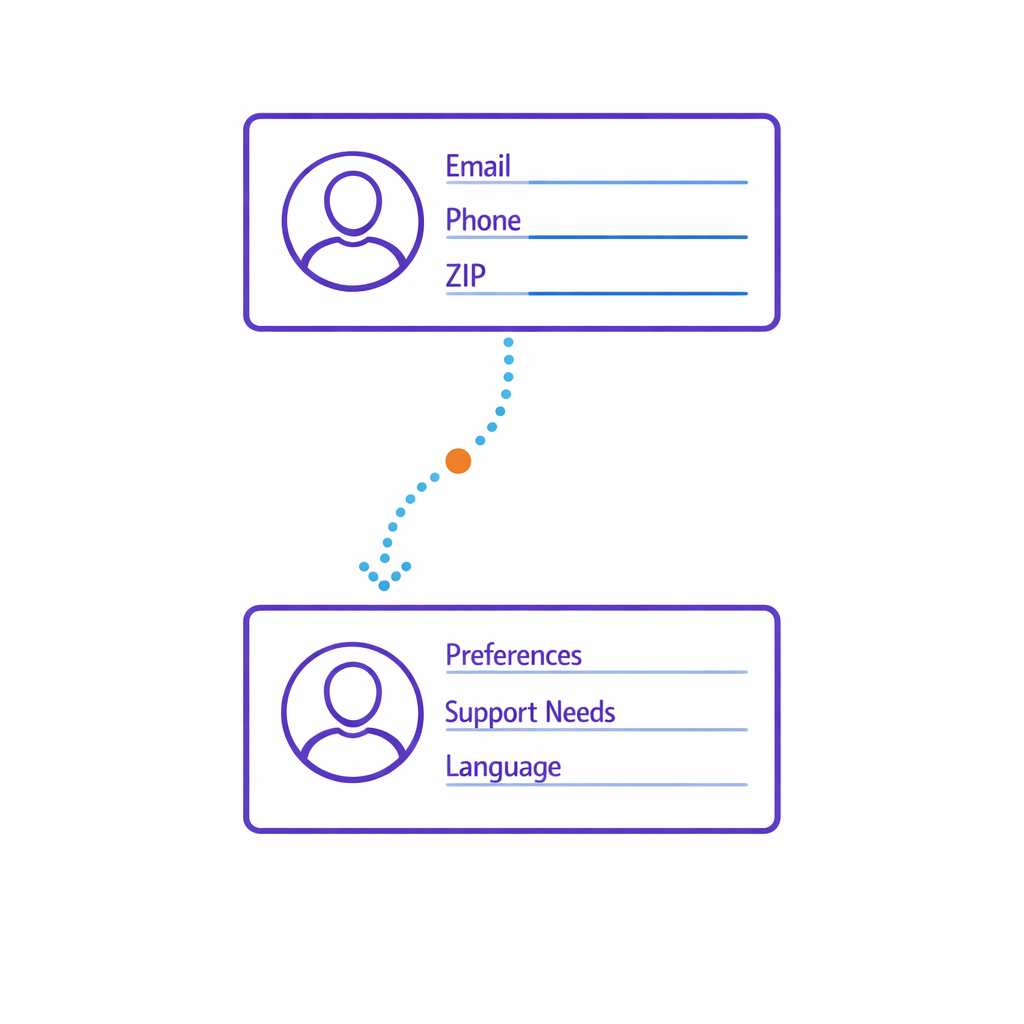
Stage 3: Identity and profile building (without forcing friction)
Identity is the bridge between enrollment and orchestration. If you cannot reliably recognize a patient across touchpoints, you cannot accurately coordinate communications, suppress duplicates, or attribute outcomes.
In practice, teams often start with a “minimum viable profile” at signup, then progressively enrich it through later steps, support interactions, or self-service preference updates. This keeps conversion high while still supporting strong patient engagement measurement later.
- Start small: collect only what you need to deliver the first value.
- Progressively enrich: ask for additional details after trust is established.
- Normalize data: format phone numbers, validate emails, and standardize key fields to reduce downstream matching issues.
Stage 4: Orchestration rules that respect consent and reduce noise
Orchestration is where omnichannel ambition often fails. Without centralized rules, channel teams end up sending overlapping messages that feel repetitive, out of sync, or irrelevant.
A healthcare engagement cloud approach typically centralizes decisioning so every downstream activation checks the same “source of truth” for consent, preferences, and eligibility. That is how you prevent the most common operational mistake: sending a message that the patient did not opt into.
- Eligibility gates: only enroll patients into journeys they qualify for right now.
- Frequency controls: cap touches across channels so you do not overwhelm the patient.
- Suppression logic: if a patient opts out, bounces, or indicates “not interested,” stop and reroute.
Stage 5: Patient education messaging that is helpful, not just compliant
Compliance-aware messaging still needs to earn attention. The most effective patient education campaigns feel like guidance, not blasts, and they deliver value in the first few touches.
For SMS patient education in particular, keep messages short, specific, and timed to the patient’s likely questions. Tie each message to the next best action, such as confirming a step, choosing a support option, or viewing a resource that answers a real barrier.
- Design for mobile reading: one idea per message, minimal jargon.
- Use sequencing: a series that builds confidence beats a long single message.
- Offer off-ramps: “reply to change preferences” or “choose email instead,” where appropriate.
Stage 6: Support handoffs that close the loop

Enrollment is only meaningful if it connects to real support. When a patient asks for help, the program should not reset their story or lose context.
Build handoffs so the support channel can see the patient’s preferences, recent messages, and the reason for the outreach. Even simple improvements like routing based on intent (“benefits question” vs. “how to take” vs. “program status”) can reduce handle time and improve patient satisfaction.
- Contextual routing: send the right requests to the right team.
- Closed-loop outcomes: record what happened, so future outreach reflects reality.
- Self-service first: let patients update preferences without calling.
Measurement that brand, ops, and compliance can all live with
Patient engagement measurement is often where teams discover they built a program that cannot be explained. The fix is to treat measurement as part of the enrollment design, not a downstream reporting project.
Start with a small set of metrics that connect directly to journey health and operational efficiency. Then make sure you can segment those metrics by consent status, channel preference, and program cohort so you can answer “what worked” without guessing.
A practical measurement framework for enrollment journeys
- Enrollment conversion: page-to-start rate, start-to-complete rate, and time to complete signup.
- Consent quality: opt-in rate by channel, preference completeness, and consent drop-off points.
- Early engagement: first-week open/click (email) and response/interaction signals (SMS), tracked at the journey level.
- Operational outcomes: reduction in manual follow-up, fewer duplicate records, fewer complaint escalations.
- Support outcomes: deflection to self-service, time to resolution, and repeat-contact rate.
When stakeholders ask for “attribution,” anchor it to the patient engagement journey rather than isolated messages. This helps avoid over-crediting a single channel and encourages smarter orchestration decisions.
Common misconceptions that create compliance and performance risk
Many enrollment and outreach problems come from reasonable assumptions that do not hold up in the real world. Addressing these early can prevent rework and uncomfortable escalations later.
Misconception 1: “If it’s educational, consent is optional.”
Even purely educational experiences should be designed with patient expectations, channel rules, and internal governance in mind. A consent-first approach reduces surprise and makes programs more resilient when scope expands or message types evolve.
Misconception 2: “We can fix consent later in CRM.”
If the source capture is unclear or incomplete, downstream systems will interpret it inconsistently. The result is manual cleanup, suppressed outreach, or messages sent without the confidence you need when legal or compliance asks for proof.
Misconception 3: “More channels automatically means more engagement.”
Omnichannel only works when the program coordinates touches across channels and respects patient preference management. Otherwise, multi-channel becomes multi-noise, and opt-outs become the leading indicator of program health.
Misconception 4: “Opt-out is a back-office workflow.”
Opt-out is part of the product. If a patient cannot easily stop or change communications, trust erodes and complaints rise, which can affect both deliverability and stakeholder confidence in the program.
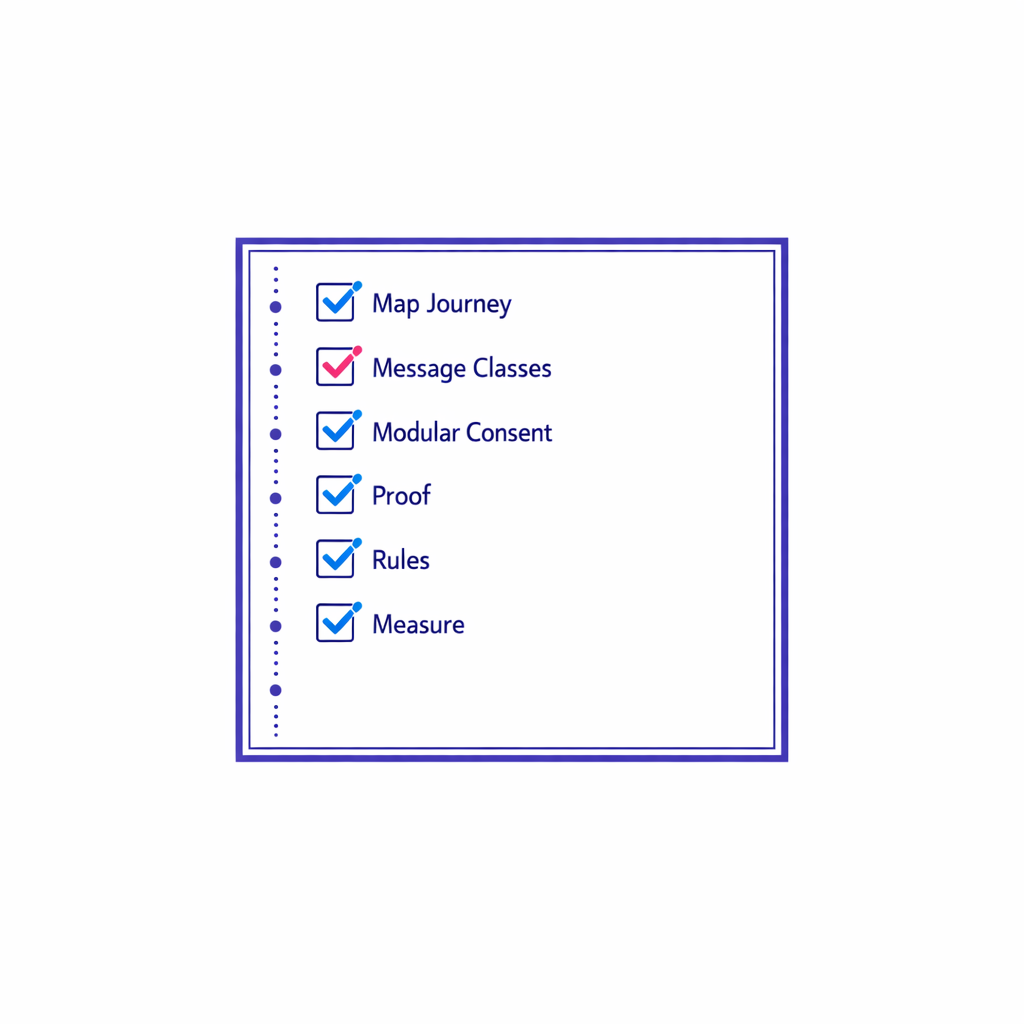
What to do next: a consent-first patient enrollment workflow checklist
If you are planning a new patient education campaign or refactoring an existing patient engagement journey, use this checklist to move from ideas to a build-ready plan. Keep it cross-functional so brand, ops, privacy, legal, and vendors align before implementation.
- Map the journey: entry points, signup steps, first 30 days of messages, and support handoffs.
- Define message classes: educational vs. support vs. promotional, and how each is governed.
- Design modular consent: purpose-based choices plus channel-based choices (email, SMS, etc.).
- Document proof requirements: what you will store as evidence of consent and preference changes.
- Set orchestration rules: eligibility, frequency caps, suppression, and conflict resolution across teams.
- Build preference management: self-service updates, easy opt-out, and clear confirmation messages.
- Define measurement upfront: enrollment conversion, consent quality, early engagement, and support outcomes.
- Operationalize governance: who owns updates, reviews, and exception handling when programs evolve.
Request a Demo: build a scalable signup-to-support journey with Pulse Health
If your team is trying to scale patient outreach omnichannel programs without losing consent integrity or measurement clarity, it helps to use a platform designed for orchestration, preference management, and program operations. Pulse Health builds infrastructure for consent-first patient engagement journeys so brand and ops teams can move faster while staying aligned to governance.
You can Request a Demo to see how a scalable patient enrollment workflow can connect signup, consent capture, patient education messaging, and support handoffs in one operational view. If you are in planning mode, you can also Book a Consultation to map your current journey, identify friction points, and define the minimum set of capabilities needed for a durable patient access platform.